LAST MEDICALLY REVIEWED:
June 2026 — Dr. Shaileshkumar Garge
Citi Vascular Hospital, KPHB Colony, Road No. 1, Hyderabad, Telangana 500072
QUICK ANSWER
FNAC vs Biopsy — Which Is Better?
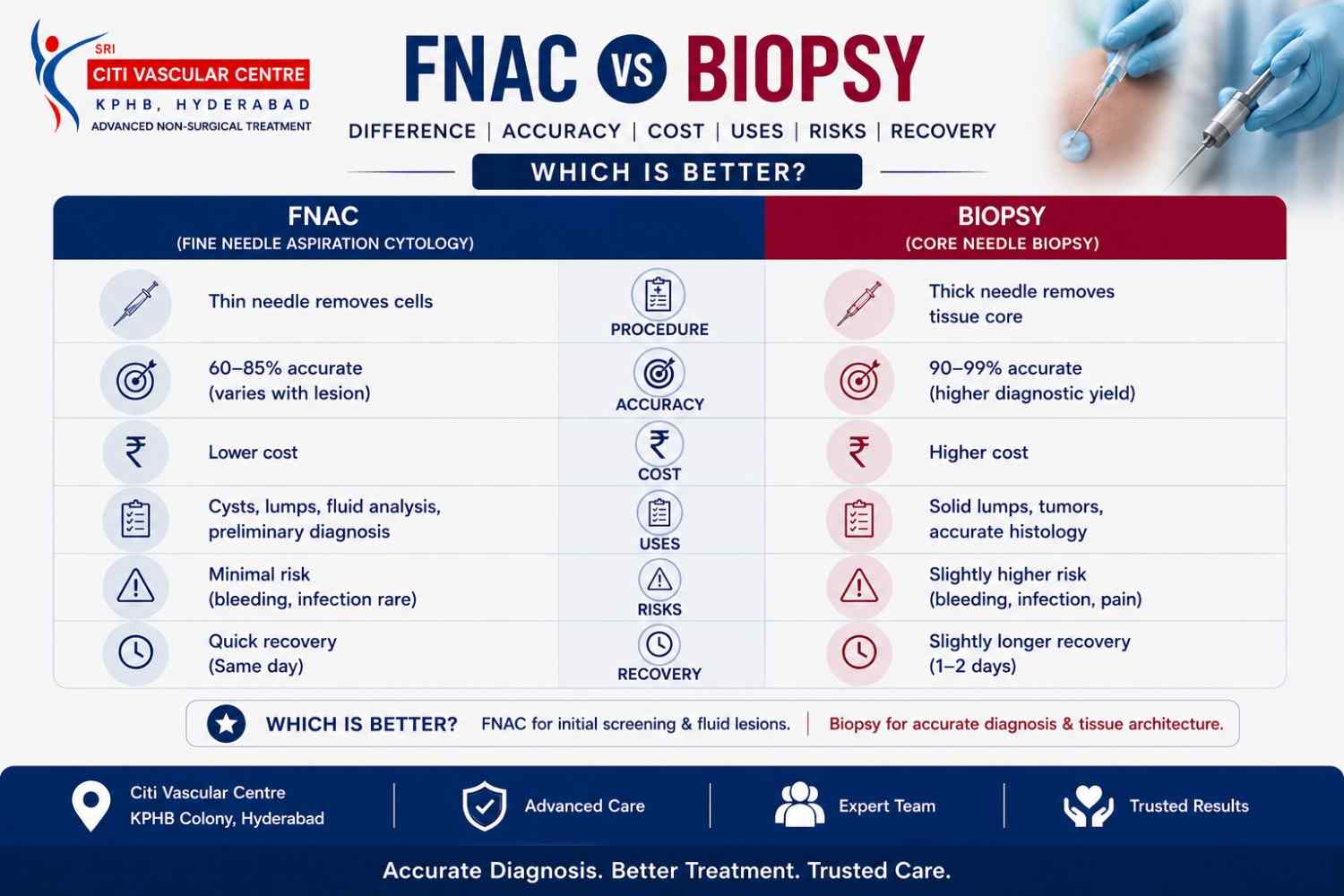
Neither is universally better — they answer different clinical questions. FNAC collects cells (cytology) using a fine needle, 10–20 minutes, usually no anaesthesia. Biopsy collects a tissue core (histology) using a cutting needle, 20–45 minutes, local anaesthesia always required. FNAC is the right first step for most accessible lesions. Biopsy is needed when tissue architecture is essential for diagnosis.
FNAC and biopsy are both minimally invasive tests used to diagnose lumps and abnormal tissues. FNAC collects individual cells using a thin needle, while a biopsy removes a small tissue sample. The best test depends on the organ, suspected condition, and the type of diagnosis required.
When a doctor recommends a diagnostic procedure for a lump or suspicious lesion, patients frequently receive the advice to have either an 'FNAC test' or a 'biopsy' — and very often have no idea what the difference between them is, or why one has been recommended over the other. The confusion is understandable. Both involve a needle. Both are minimally invasive. Both produce a laboratory report. And in both cases the goal is the same: to find out what the abnormal tissue is made of, so that the right treatment can be planned.
The difference, however, is clinically significant. FNAC and core needle biopsy are not interchangeable tests. They collect different things, provide different levels of diagnostic information, involve different levels of discomfort and preparation, and cost different amounts. Choosing the wrong test for a given clinical situation — or choosing the cheaper one without understanding what it can and cannot diagnose — can delay your diagnosis and result in a second procedure anyway. This guide explains both tests clearly and completely, compares them across every dimension that matters to a patient in Hyderabad in 2026, and helps you understand which one is right for your specific situation.
FNAC and Core Needle Biopsy — Both Available at Citi Vascular Centre, KPHB, Hyderabad
Call +91-73375 83901 | WhatsApp 73375 83901 | citivascularcentre.com | Mon–Sat 9AM–6PM
|
Feature |
FNAC (Fine Needle Aspiration) |
Core Needle Biopsy |
|
What Is Collected |
Individual cells — cytology |
Tissue cylinder — histology + architecture |
|
Needle Type |
Fine aspiration needle: 21–25 gauge |
Cutting needle: 14–18 gauge |
|
Anaesthesia |
Often not required |
Always required — local anaesthetic to skin and tract |
|
Duration |
10–20 minutes |
20–45 minutes |
|
Pain Level |
Minimal — comparable to blood test |
Mild to moderate — controlled with local anaesthesia |
|
Result Turnaround |
2–5 days (cytology report) |
3–7 days histopathology | Up to 14 days with IHC |
|
Post-Procedure Observation |
20–30 minutes |
2–6 hours depending on organ |
|
Hospital Admission |
Not required — day care |
Not required — day care for most procedures |
|
Blood Tests Needed |
Usually not required |
Required for deep organ biopsies — INR, platelets, FBC |
|
Blood Thinners — Pause? |
Usually not required to pause |
Must be paused before biopsy — drug-specific timing |
|
Can Sub-Type Lymphoma |
No — insufficient tissue for sub-typing |
Yes — IHC panel provides full lymphoma classification |
|
Can Grade Prostate Cancer |
No |
Yes — Gleason/ISUP grade from tissue cores |
|
Molecular Profiling (EGFR, PD-L1) |
Limited — small cell numbers |
Yes — adequate tissue for all molecular markers |
|
Indicative Cost — Hyderabad 2026 |
Rs 3,000–20,000 |
Rs 6,000–30,000 |
|
Best For |
Thyroid nodules | Breast lumps | Lymph nodes (non-lymphoma) | First-line for most accessible lesions |
After inconclusive FNAC | Lymphoma | Prostate | Bone | Sarcoma | Molecular profiling needed |
The bottom line: FNAC is the right first step for most accessible lesions where cytology is sufficient for diagnosis. Biopsy is the right first step — or the necessary next step after FNAC — when tissue architecture, sub-typing, or molecular profiling is required. Dr. Garge advises which test is right for your specific lesion after reviewing your imaging at Citi Vascular Centre, KPHB. Call +91-73375 83901.
FNAC stands for Fine Needle Aspiration Cytology. It is a minimally invasive diagnostic procedure in which a very thin hollow needle — typically 21 to 25 gauge, significantly finer than a standard injection needle — is guided into a lump or lesion and used to draw out a small number of cells through gentle suction. Those cells are placed on a glass slide, stained with appropriate dyes, and examined under a microscope by a cytopathologist, who identifies what type of cells are present and whether they appear benign, malignant, inflammatory, or infectious.
The critical word in FNAC is 'cytology' — the study of individual cells. FNAC gives the pathologist individual cells to examine, but not the structural framework of the tissue those cells came from. This is sufficient to answer many diagnostic questions — is this thyroid nodule benign or malignant? Is this lymph node enlarged because of infection or cancer? Is this breast lump a fibroadenoma or a carcinoma? — but it is not sufficient for diagnoses that require knowing how cells are arranged within the tissue architecture, such as lymphoma sub-typing or prostate cancer grading.
USG-guided FNAC — performed under real-time ultrasound — is the modern standard. The operator watches the needle on the ultrasound screen as it advances into the lesion, confirming precise placement before aspiration begins. This dramatically improves accuracy for small, deep, or complex lesions compared with older palpation-guided techniques.
Core needle biopsy (CNB) is a minimally invasive diagnostic procedure in which a spring-loaded or vacuum-assisted cutting needle — typically 14 to 18 gauge — is advanced into a lesion under image guidance and fires through the target, extracting a small cylindrical core of tissue approximately 1–2mm in diameter and 10–20mm in length. This tissue core is processed, sliced thinly, stained, and examined histopathologically — the pathologist can see not just individual cells but how they are arranged within the tissue, what structures they form, and what proteins they express through special staining techniques (immunohistochemistry — IHC).
The key word here is 'histology' — the study of tissue structure. This structural information is what makes core needle biopsy diagnostically more powerful than FNAC for certain conditions. When the diagnosis requires knowing the tumour grade, the specific lymphoma sub-type, the hormone receptor status of a breast cancer, or the EGFR mutation status of a lung cancer for targeted therapy — these answers come from histology with IHC, not from cytology alone.
Core needle biopsy is always performed under image guidance at Citi Vascular Centre — real-time ultrasound for accessible organs, CT guidance for deep or osseous lesions. Local anaesthesia is always used to numb the skin and needle tract. Two to four tissue cores are taken from different parts of the lesion to ensure representative sampling.
The differences between FNAC and core needle biopsy go beyond needle size. Understanding them helps explain why one test is recommended over the other in specific clinical situations — and why trying to use FNAC for a diagnosis that needs biopsy tissue will almost always result in an inconclusive report and a second procedure.
|
The Difference |
How FNAC Handles It |
How Biopsy Handles It |
|
What is sampled |
Loose cells aspirated from the lesion surface or interior — no tissue structure preserved |
A cylindrical tissue core removed from the lesion — cellular architecture fully preserved for histological examination |
|
Lymphoma diagnosis |
Can suggest lymphoma — but cannot sub-type. DLBCL vs Hodgkin vs Follicular vs Mantle Cell require IHC on tissue, not cytology. |
Full IHC panel on tissue core provides definitive lymphoma sub-typing — determines which chemotherapy protocol is used |
|
Cancer grading |
Can identify malignant cells — cannot grade. Grade requires structural tumour architecture. |
Gleason/ISUP grade for prostate | Nottingham grade for breast | all require tissue architecture |
|
Molecular markers |
Limited cell numbers restrict molecular testing. EGFR, ALK, PD-L1 testing possible but less reliable than tissue. |
Adequate tissue for IHC, FISH, PCR, and next-generation sequencing of molecular markers |
|
Fibrosis staging |
Cannot stage liver fibrosis — cytology shows cells but not fibrous tissue architecture |
Core biopsy essential for liver fibrosis staging (Metavir/Ishak) — fibrous bands only visible on tissue section |
|
Sarcoma sub-typing |
Can suggest spindle cell neoplasm — cannot classify sarcoma sub-type for surgical planning |
Histology + IHC classifies liposarcoma vs leiomyosarcoma vs synovial sarcoma — critical for correct surgical margin planning |
|
Adequacy rate |
5–15% inadequate samples — higher for fibrous, very small, or mainly cystic lesions |
< 5% inadequate when image-guided — mechanical cutting provides tissue regardless of cellularity |
FNAC vs Biopsy Accuracy – Key Points:
Accuracy comparisons between FNAC and biopsy require context — because accuracy depends on both the type of lesion being tested AND the diagnostic question being asked. For many common applications, FNAC is highly accurate. For specific diagnoses that require tissue architecture, FNAC is not inaccurate — it is structurally incapable of providing the answer, regardless of how well the procedure is performed.
|
Application |
FNAC Accuracy |
Biopsy Accuracy |
Inadequate Rate |
Preferred Test |
|
Thyroid nodule (benign vs malignant) |
85–95% sensitivity |
95–98% |
5–15% FNAC |
FNAC first — Bethesda III/IV → biopsy |
|
Breast lump (benign vs malignant) |
80–90% sensitivity |
95–98% |
5–10% FNAC |
FNAC first — inconclusive → core biopsy |
|
Cervical lymph node — TB |
70–90% (cytology + ZN stain) |
95–98% (granuloma + culture) |
Moderate |
FNAC first — inconclusive → biopsy |
|
Lymphoma — detection |
80–90% can suggest lymphoma |
95–98% |
Moderate |
Sub-typing always needs biopsy |
|
Lymphoma — sub-typing |
Not possible reliably |
95–98% with full IHC |
N/A |
Biopsy — mandatory for sub-typing |
|
Liver mass — HCC |
80–90% |
90–95% |
Variable |
Either — based on imaging and clinical context |
|
Liver fibrosis staging |
Not possible |
95%+ (Metavir/Ishak) |
N/A |
Biopsy — mandatory |
|
Lung cancer — diagnosis |
80–90% |
90–95% |
10–15% |
Biopsy preferred for molecular markers |
|
Prostate cancer — grading |
Not applicable |
95%+ |
N/A |
MRI-targeted biopsy mandatory |
|
Soft tissue sarcoma |
Can suggest malignancy — cannot sub-type |
95%+ with IHC |
High for sub-typing |
Core biopsy — mandatory for sarcoma |
What 'inaccurate FNAC' usually means: When patients receive an inconclusive or inadequate FNAC result, it is not usually because the procedure was poorly performed — it is because the lesion type produces cells that are difficult to interpret on cytology alone (follicular thyroid lesions, lymphoma, highly fibrous lesions). In these cases, biopsy is not a fallback for a failed FNAC — it is the diagnostically appropriate test for that type of lesion.
The right choice between FNAC and biopsy varies significantly by organ. For some sites, FNAC is well-established as the standard first-line test and biopsy is reserved for specific situations. For other sites, biopsy is the recommended approach from the outset. The table below gives organ-specific guidance.
|
Organ |
FNAC Role |
Biopsy Role |
When to Escalate to Biopsy |
|
Thyroid |
First-line for nodules > 1cm. Bethesda I–VI classification. |
Bethesda III–IV (follicular lesion) | Inconclusive cytology | Before lobectomy decision |
FNAC Bethesda IV → biopsy or lobectomy | Bethesda V–VI → surgery directly |
|
Breast |
Part of triple assessment — rapid diagnosis of breast lump |
When FNAC is inconclusive | Hormone receptor status needed | Microcalcifications (VAB preferred) |
Any breast malignancy diagnosis needs biopsy for ER/PR/HER2 status before treatment planning |
|
Lymph Node |
First-line for most lymphadenopathy — screens for TB, reactive, metastatic |
Lymphoma suspected | FNAC inconclusive or suggests lymphoid malignancy |
Any suggestion of lymphoma on FNAC → biopsy mandatory for sub-typing |
|
Liver |
Rapid diagnosis of hepatic mass — metastasis, HCC, benign |
Liver fibrosis staging | Inconclusive FNAC | Hepatocellular carcinoma with IHC needed |
Fibrosis staging always needs biopsy | HCC where IHC for primary identification required |
|
Kidney |
Selected cases — rapid screening of renal mass |
RCC vs oncocytoma vs AML distinction | Any renal mass where histology changes management |
When benign histology (oncocytoma) would avoid surgery — biopsy direct saves FNAC step |
|
Lung |
Possible for peripheral lesions — diagnosis of malignancy vs benign |
Preferred — NSCLC sub-typing + EGFR/ALK/PD-L1 needed for targeted therapy selection |
Lung cancer always needs biopsy for molecular profiling even if FNAC confirms malignancy |
|
Salivary Gland |
First-line — benign (pleomorphic adenoma, Warthin) vs carcinoma |
Carcinoma on FNAC → confirms type before surgery |
Carcinoma on FNAC → core biopsy or direct surgical excision |
|
Bone |
Limited role — mainly for accessible lytic lesions confirming metastasis |
Primary bone tumour | Bone metastasis needing primary identification | Vertebral lesion |
Most bone lesions go directly to CT-guided trephine biopsy — FNAC rarely adequate for bone |
|
Soft Tissue |
Can screen superficial lumps — lipoma vs sarcoma screening |
Any suspicion of sarcoma | Histology + IHC mandatory for sarcoma sub-typing |
Any complex or heterogeneous soft tissue mass → biopsy direct | Sarcoma suspected → biopsy mandatory |
|
Prostate |
Not a standard approach for prostate |
MRI-targeted biopsy for PI-RADS 4–5 lesions | Gleason grade essential for treatment planning |
Biopsy is the only appropriate test for prostate cancer diagnosis and grading |
Concern about pain is one of the most common reasons patients delay seeking a diagnostic procedure. Understanding what each test actually feels like — with honesty about the differences — helps patients arrive with realistic expectations rather than either unnecessary fear or false reassurance.
|
Pain Aspect |
FNAC Experience |
Core Needle Biopsy Experience |
|
Needle Size |
21–25G — thinner than a blood test needle |
14–18G — larger, with spring-loaded cutting mechanism |
|
Anaesthesia Given |
Often none for superficial sites. Optional topical cream. Some sites: 1 small injection. |
Always: local anaesthetic to skin + needle tract. Sedation available for bone and deep organs. |
|
During the Procedure |
Brief sting 2–3 seconds. Mild pressure during aspiration. Most patients say less than expected. |
Pressure and brief dull sensation when needle fires (0.1 seconds). Tract is numbed before this. |
|
Post-Procedure Day 0 |
Minimal or none. Small plaster. Walk to car and drive home. |
Mild to moderate aching at biopsy site. Paracetamol manages well for most patients. |
|
Post-Procedure Day 1–2 |
No ongoing discomfort expected. Normal activities. |
Aching reducing. Bruise may appear. Most patients comfortable by Day 2. |
|
Most Painful Part |
The anticipation. Most patients leave saying it was easier than a blood test. |
The local anaesthetic injections (multiple for deep organ biopsies). The cutting itself is not felt. |
|
Overall Pain Rating |
1–2 / 10 for superficial sites |
2–4 / 10 with local anaesthesia well-administered. Bone biopsy: 3–4 / 10 with sedation. |
Needle-anxious patients: if you are concerned about multiple needle injections, FNAC is the significantly less intimidating option: often no anaesthetic injections at all, and the fine needle is far smaller than any standard medical needle. For biopsy, the local anaesthetic injections (not the biopsy needle itself) are the main source of discomfort — and these can be minimised with slow, careful injection technique.
|
Risk Category |
FNAC — Risk Profile |
Core Needle Biopsy — Risk Profile |
|
Pain and bruising |
Very common — mild and brief. Resolves within 24–48 hours. |
Common — mild to moderate. Resolves within 1–3 days with paracetamol. |
|
Significant bleeding |
Very rare — fine needle creates minimal vessel disruption |
0.5–2% for deep organ biopsies. Doppler maps vessels before needle placement. |
|
Pneumothorax (lung procedures only) |
1–5% for lung FNAC |
5–15% for CT-guided lung biopsy. Post-procedure chest X-ray standard. |
|
Infection |
< 0.5% — sterile technique prevents this |
< 1% — sterile technique. Antibiotics if confirmed. |
|
Vasovagal faintness |
Uncommon — more in anxious patients |
Uncommon — managed immediately with positioning |
|
Needle track seeding |
Extremely rare — theoretical concern for specific tumour types |
Extremely rare — biopsy tract planned along future surgical excision axis for sarcoma cases |
|
Blood thinners required to stop |
Usually not necessary — fine needle rarely needs anticoagulant pause |
Yes — aspirin 5–7 days | clopidogrel 5–7 days | warfarin 5 days | NOACs 48–72 hours |
|
Blood tests required pre-procedure |
Usually not — may be needed for deep organ FNAC |
Required for all deep organ biopsies — FBC, PT/INR, APTT, platelet count |
|
Overall risk profile |
Very low — one of the safest diagnostic procedures in medicine |
Low but higher than FNAC — proportional to the organ being biopsied and depth of access |
|
Recovery Stage |
After FNAC |
After Core Needle Biopsy |
|
Immediately after |
20–30 min observation. Small plaster. Most patients drive themselves home. |
2–6 hours observation. Post-biopsy imaging scan. Arrange a driver — especially for deep organ. |
|
Day 0 evening |
Normal activities — cooking, working from home, light tasks. No restrictions. |
Rest at home. Paracetamol as needed. Light meals. No strenuous activity. |
|
Day 1–2 |
Fully normal. Return to office, driving, exercise. Zero restrictions for most patients. |
Superficial biopsy: normal activities Day 1. Deep organ biopsy: light activities Day 1–2, office from Day 2–3. |
|
Day 3–7 |
Nothing — awaiting result. Full normal life. |
Normal life resumed. Aching resolved. Await histopathology result. |
|
Return to office work |
Same day or next day for almost all patients |
Day 1–2 (superficial) | Day 2–4 (deep organ) |
|
Return to physical work |
Same day in most cases |
Day 3–7 depending on organ and site |
|
Result available |
2–5 days — cytology report |
3–7 days — histopathology | Up to 14 days with IHC staining |
|
Overall recovery |
Fastest — no meaningful recovery period for most patients |
Longer but still far less than surgical biopsy under general anaesthesia |
FNAC vs Biopsy Cost – Quick Summary:
Biopsy costs more than FNAC of the same organ for three clear reasons: the cutting needle is larger and the device itself is more expensive; the tissue core requires histopathological processing rather than cytological slide preparation; and the procedure takes longer with greater clinical resource requirements. The cost difference is not arbitrary pricing — it reflects the genuine difference in what each procedure involves.
|
Organ |
FNAC Cost — Citi Vascular, KPHB |
Core Biopsy Cost — Citi Vascular, KPHB |
|
Thyroid |
Rs 3,000–7,000 |
Not standard first-line — molecular lobectomy for Bethesda IV |
|
Breast |
Rs 3,500–8,000 |
Rs 8,000–18,000 | Vacuum-assisted: Rs 15,000–30,000 |
|
Lymph Node |
Rs 3,000–7,000 |
Rs 7,000–15,000 (incl. IHC for lymphoma sub-typing) |
|
Liver |
Rs 5,000–12,000 |
Rs 8,000–18,000 |
|
Kidney |
Rs 6,000–15,000 |
Rs 10,000–20,000 |
|
Lung |
Rs 10,000–20,000 |
Rs 15,000–28,000 (incl. CT + IHC molecular markers) |
|
Bone |
Rs 10,000–20,000 (CT-guided) |
Rs 18,000–30,000 (CT + trephine + sedation) |
|
Soft Tissue |
Rs 3,500–8,000 |
Rs 8,000–16,000 (incl. IHC for sarcoma sub-typing) |
The false economy of choosing FNAC to save money when biopsy is clinically needed: If lymphoma is suspected, ordering FNAC to save Rs 5,000–8,000 will almost certainly return a result of 'lymphoma cells present but sub-typing not possible on cytology' — followed by a biopsy anyway. The total cost of FNAC + biopsy is higher than direct biopsy. Dr. Garge advises the right test first time at consultation. WhatsApp 73375 83901.
The right test depends on your clinical situation, not a general preference. Here is a decision guide based on the most common clinical scenarios patients present with at Citi Vascular Centre, KPHB, Hyderabad.
|
Your Situation |
Recommended First Test |
Reason |
|
Thyroid nodule > 1cm found on ultrasound |
FNAC |
Standard first-line — Bethesda classification guides surgery vs surveillance |
|
Breast lump — need to know benign or malignant |
FNAC |
Part of triple assessment. Quick, minimally invasive screening. |
|
Breast lump confirmed malignant on FNAC — treatment planning |
BIOPSY |
ER/PR/HER2 status required before surgery, chemotherapy, or radiotherapy planning |
|
Enlarged lymph nodes — first evaluation |
FNAC |
Screens for TB, reactive, metastatic. Fast, minimal discomfort. |
|
Lymphoma suspected on FNAC or imaging |
BIOPSY |
Sub-typing mandatory — DLBCL vs Hodgkin vs Follicular determines chemotherapy protocol |
|
Liver mass — identify type |
FNAC |
Adequate for most hepatic mass diagnosis without the cost of biopsy as first step |
|
Liver disease — staging fibrosis |
BIOPSY |
Cytology cannot stage fibrosis — tissue architecture essential for Metavir/Ishak scoring |
|
Lung nodule — is it cancer and what type? |
BIOPSY |
Sub-type + molecular markers (EGFR, ALK, PD-L1) needed for targeted therapy — biopsy provides adequate tissue |
|
Bone lesion of uncertain nature |
BIOPSY |
CT-guided trephine biopsy — most bone lesions need histology, not cytology |
|
Prostate cancer diagnosis — rising PSA, suspicious MRI |
BIOPSY |
MRI-targeted biopsy for Gleason grading — cytology not appropriate for prostate |
|
Soft tissue lump — is it a sarcoma? |
BIOPSY |
Sarcoma sub-typing mandatory before surgery — wrong sub-type = inadequate surgical margin |
|
Previous FNAC returned inconclusive or inadequate result |
BIOPSY |
Core biopsy provides tissue regardless of cellularity — resolves most inconclusive cytology |
|
FNAC showed malignancy — need molecular profiling for targeted therapy |
BIOPSY |
EGFR, ALK, KRAS, PD-L1, HER2 — adequate tissue from biopsy for all molecular markers |
Yes — and this is sometimes the most efficient approach. In specific clinical situations, Dr. Garge may recommend performing both an FNAC and a core needle biopsy at the same visit, or may perform core biopsy in the same session where FNAC was originally planned if the initial approach suggests biopsy will be needed. Examples where combined same-session sampling is considered:
|
Scenario |
How Combined Sampling Helps |
|
Suspected lymphoma — first visit |
FNAC for immediate cytological screening + core biopsy for definitive sub-typing performed in the same session — eliminates a return visit |
|
Breast mass where FNAC is expected to show malignancy |
FNAC for rapid cytological confirmation + core biopsy for hormone receptor status in the same appointment — treatment planning begins immediately |
|
Liver mass where both cytology and fibrosis staging are needed |
FNAC for cellular characterisation of the mass + core biopsy for fibrosis staging — both completed in one procedure |
|
Multiple lesions requiring different sampling approaches |
FNAC for a superficial accessible lesion + core biopsy for a deeper or more complex co-existing lesion — all in one clinic visit, one preparation, one set of blood tests |
Practical benefit of same-session combined sampling: For patients who have come from another city (Warangal, Nizamabad, Andhra Pradesh) or who have taken a day off work, completing FNAC and biopsy in one visit eliminates the need to travel back for a second procedure. Dr. Garge will advise at your consultation if combined sampling in one visit is appropriate for your specific situation. Call +91-73375 83901
Image-guided FNAC and biopsies are commonly performed by interventional radiologists or other specialists trained in image-guided procedures. The choice depends on the organ involved and the clinical indication.
|
Credential / Feature |
Detail |
|
Qualifications |
MBBS | MD (Mumbai) | DNB (Delhi) | FRCR (UK) | FNVIR (CMC Vellore) | EBIR (Spain/Europe) | Fellowship (North Carolina, USA) |
|
Role |
Director and Chief Vascular Physician | Senior Consultant Vascular and Interventional Radiologist |
|
Experience |
12+ years dedicated interventional radiology | 15,000+ image-guided diagnostic procedures |
|
Both Tests Available |
FNAC + Core Needle Biopsy + Vacuum-Assisted Biopsy + Bone Trephine Biopsy — all under image guidance at KPHB |
|
Right Test First Time |
Dr. Garge advises FNAC vs biopsy based on your imaging and clinical picture — not a default protocol applied to every patient |
|
One-Stop Visit |
Imaging review + FNAC or biopsy + post-procedure scan + result follow-up — all with the same specialist, one appointment |
|
Transparent Pricing |
Itemised cost estimate provided before you commit. Insurance assistance. 0% EMI for eligible patients. |
Q1: What is the difference between FNAC and biopsy?
FNAC (Fine Needle Aspiration Cytology) uses a very fine needle (21–25G) to collect loose cells for cytological examination. Core needle biopsy uses a larger cutting needle (14–18G) to extract a cylindrical tissue core for histopathological examination. FNAC provides individual cells — quick, usually no anaesthesia needed. Biopsy provides tissue architecture — more diagnostic detail, always requires local anaesthesia. The right test depends on which diagnostic question needs to be answered.
Q2: Which is more accurate — FNAC or biopsy?
For most accessible lesions (thyroid, breast, lymph nodes, liver), FNAC achieves 80–95% diagnostic accuracy — sufficient for many clinical decisions. Core needle biopsy achieves 90–98% accuracy and is more reliable for complex diagnoses. For specific diagnoses requiring tissue architecture — lymphoma sub-typing, prostate cancer grading, liver fibrosis staging, sarcoma classification — FNAC cannot provide the answer regardless of accuracy, because the structural information simply is not there in individual cells.
Q3: Is FNAC or biopsy more painful?
FNAC is significantly less uncomfortable than biopsy. FNAC uses a very fine needle (thinner than a blood test needle) and typically requires no anaesthetic at all for superficial sites. Most patients rate it 1–2 out of 10. Core needle biopsy uses a larger cutting needle and always requires local anaesthetic injections to numb the tract — the main discomfort source. Post-biopsy aching lasts 4–24 hours. Overall rating: 2–4 out of 10 with good anaesthesia.
Q4: When is biopsy needed instead of FNAC?
Biopsy is needed instead of FNAC when: lymphoma sub-typing is required (cytology cannot sub-type lymphoma reliably), prostate cancer Gleason grading is needed, liver fibrosis requires staging, soft tissue sarcoma sub-typing is required for surgical planning, molecular profiling (EGFR, ALK, PD-L1, HER2) is needed for targeted therapy, or a previous FNAC has returned inconclusive or inadequate. For any of these situations, proceeding directly to core needle biopsy avoids a second procedure.
Q5: Can FNAC detect cancer?
Yes — FNAC can detect cancer in most accessible lesions with 80–95% sensitivity. A malignant FNAC result means cancerous cells have been identified. However, FNAC alone cannot usually determine the specific cancer sub-type or grade needed for treatment planning — most cancer treatment decisions require a follow-up core needle biopsy for hormone receptor status, molecular marker testing, or definitive histological classification before therapy begins.
Q6: What happens if FNAC is inconclusive?
An inconclusive FNAC result — either inadequate (too few cells) or indeterminate (atypical cells that cannot be classified) — is not unusual, occurring in 5–15% of procedures. The next step is core needle biopsy, which provides a tissue core that can be diagnosed regardless of cellularity. At Citi Vascular Centre, KPHB, if the FNAC sample is macroscopically inadequate before you leave, an additional pass is made in the same visit — or a core biopsy is recommended immediately.
Q7: What is the cost difference between FNAC and biopsy in Hyderabad?
FNAC costs Rs 3,000–20,000 in Hyderabad depending on the organ and imaging modality. Core needle biopsy costs Rs 6,000–30,000 for the same range of organs. The cost difference reflects: a larger and more expensive cutting needle, histopathological processing (vs cytology), longer procedure time, always-required local anaesthesia, extended post-procedure observation, and blood tests required before deep organ biopsy. IHC staining panels for biopsy sub-typing may add further costs depending on the panel required.
Q8: Do I need to fast before FNAC or biopsy?
For FNAC of superficial sites (thyroid, breast, lymph nodes, soft tissue) — no fasting is required. For deep organ FNAC or biopsy (liver, kidney, lung, retroperitoneum, bone) — 4–6 hours fasting before the procedure is recommended for patient comfort and safety. For bone biopsy with IV sedation — 6 hours fasting is standard. Dr. Garge's team provides specific fasting instructions when you book your appointment. When in doubt, WhatsApp 73375 83901 to confirm.
Q9: Can FNAC and biopsy be done on the same day?
Yes — in specific clinical situations, Dr. Garge performs FNAC and core needle biopsy in the same session at Citi Vascular Centre, KPHB. This is particularly useful when: lymphoma is suspected (FNAC for cytology + biopsy for sub-typing), breast malignancy is likely (FNAC for confirmation + biopsy for hormone receptors), or multiple lesions need different sampling approaches. Same-session combined sampling eliminates a return visit — especially valuable for outstation patients from Warangal, Nizamabad, and Andhra Pradesh.
Q10: Do I need to stop blood thinners before FNAC or biopsy?
For most FNAC procedures of superficial sites — blood thinners do not need to be stopped. For core needle biopsy or deep organ FNAC — blood thinners must be paused beforehand. Specific pause durations: aspirin 5–7 days | clopidogrel 5–7 days | warfarin 5 days (INR confirmed before procedure) | apixaban and rivaroxaban 48–72 hours. Never stop anticoagulants without medical guidance. Dr. Garge's team provides written medication instructions when you book. WhatsApp 73375 83901.
Q11: Which is better for thyroid nodule — FNAC or biopsy?
FNAC is the standard first-line test for thyroid nodules and is recommended by all major international guidelines (NICE, ATA, ETA). The Bethesda System classifies FNAC results into 6 categories guiding management. FNAC is sufficient for most thyroid diagnoses. Core needle biopsy is recommended for Bethesda III–IV results (follicular lesion, indeterminate), where cytology cannot distinguish adenoma from carcinoma and tissue architecture is needed to guide the surgery vs surveillance decision.
Q12: Who is the best doctor for FNAC and biopsy in Hyderabad?
Dr. Shaileshkumar Garge — FRCR (UK), FNVIR (CMC Vellore), EBIR (Spain) — Director and Chief Vascular Physician at Citi Vascular Centre, KPHB Colony, Hyderabad, performs both USG and CT-guided FNAC and core needle biopsy with 12+ years of dedicated interventional radiology experience and 15,000+ image-guided procedures. He advises which test is right for your specific lesion after reviewing your imaging — not a default protocol. Call +91-73375 83901 or WhatsApp 73375 83901.
Q13: Which is the best hospital or centre for FNAC and biopsy in Hyderabad?
Citi Vascular Centre, KPHB Colony, Road No. 1, Hyderabad, is one of the most credentialled centres for both FNAC and core needle biopsy in the city. Led by Dr. Shaileshkumar Garge — FRCR (UK), FNVIR (CMC Vellore), EBIR (Spain) — with 15,000+ image-guided procedures, the centre offers USG and CT-guided FNAC and biopsy for all organs, with histopathology, IHC, transparent pricing, and same-day discharge. Call +91-73375 83901 or WhatsApp 73375 83901.
FNAC AND BIOPSY IN HYDERABAD
Citi Vascular Centre, KPHB Colony, Road No. 1, Hyderabad — FNAC and core needle biopsy for all organs, available for patients from:
Kukatpally and KPHB — 5 min
Miyapur and Bachupally — 10 min
Hitech City, Madhapur and Ameerpet — 20 min
Gachibowli, Kondapur and Banjara Hills — 25 min
Secunderabad and Begumpet — 25 min
Kompally, Medchal and Alwal — 20–25 min
Telangana and Andhra Pradesh — outstation welcome
|
Centre |
Contact |
Hours and Booking |
|
Citi Vascular Centre |
+91-73375 83901 |
KPHB Colony, Road No. 1, Hyderabad, Telangana 500072 | Mon–Sat 9AM–6PM |
|
WhatsApp Enquiry |
73375 83901 |
Send imaging report for advice on FNAC vs biopsy + personalised cost estimate | Same-week appointments |
SUMMARY
FNAC and core needle biopsy are complementary tools in the diagnostic pathway — not competing alternatives. FNAC is the right starting point for most accessible lesions because it is quick, requires no anaesthesia for superficial sites, produces results in 2–5 days, and answers the most common clinical questions (benign vs malignant, infection vs cancer, reactive vs lymphoma) with 80–95% accuracy. Core needle biopsy is the right choice when the diagnosis requires tissue architecture: lymphoma sub-typing, prostate grading, liver fibrosis staging, sarcoma classification, or molecular profiling for targeted cancer therapy.
Understanding the difference helps you arrive at your consultation informed — knowing why your doctor has recommended one over the other, what the procedure will feel like, how long recovery takes, and what the result will tell you. At Citi Vascular Centre, KPHB Colony, Hyderabad, both FNAC and core needle biopsy are available under real-time image guidance by Dr. Shaileshkumar Garge — FRCR (UK), FNVIR (CMC Vellore), EBIR (Spain). Where possible, combined FNAC and biopsy in one session is offered to eliminate unnecessary return visits. If you are unsure which test is right for your situation, WhatsApp your imaging report to 73375 83901 and Dr. Garge's team will advise before you book.
FNAC or Biopsy — Get the Right Test First Time
USG and CT-Guided FNAC + Core Needle Biopsy | All Organs | One Appointment
Dr. Shaileshkumar Garge | FRCR (UK) | FNVIR (CMC Vellore) | EBIR (Spain) | 12+ Years | 15,000+ Procedures
Call +91-73375 83901 | WhatsApp 73375 83901 | citivascularcentre.com
Transparent Pricing | Insurance Assisted | 0% EMI Available | Same-Day Discharge | Mon–Sat 9AM–6PM